Cancer Pain: Interventional Approaches for Better Comfort
Cancer pain can be severe and persistent. When oral medication is not enough, interventional procedures offer a targeted approach to dramatically reduce pain and improve quality of life.
Cancer pain affects up to 80 percent of patients with advanced disease. Interventional pain procedures work alongside, and not instead of, your oncology team, often achieving control where oral medication alone has fallen short.
What is Cancer Pain?
Cancer pain can arise from the tumour pressing on nerves, bones, or organs; from the treatments used to fight cancer; or from both. It can be nociceptive (arising from tissue damage), neuropathic (arising from nerve injury), or a mixture of both.
The WHO Analgesic Ladder guides the escalation of oral pain medication from paracetamol to mild opioids to strong opioids. When pain persists despite adequate oral treatment, or when side effects from opioids become unacceptable, interventional procedures are the appropriate next step.
These procedures are not a last resort. Early interventional input can reduce total opioid requirements, lessen side effects such as constipation and sedation, and make a significant difference to a patient's quality of life.

Presentations of Cancer Pain
Cancer pain presents in several distinct ways:
- Persistent aching or gnawing pain at the tumour site or in affected organs
- Breakthrough pain: sudden, severe pain episodes occurring despite regular background medication
- Burning or shooting neuropathic pain along nerve pathways from tumour invasion or chemotherapy
- Bone pain from metastases, typically worse at night and with movement
- Deep abdominal or pelvic pain from visceral nerve involvement
- Post-surgical or post-radiotherapy pain from scar tissue and nerve changes
- Opioid-related side effects that limit adequate medication dosing
A detailed pain assessment is the starting point of every consultation. Characterising the type and location of pain precisely guides which interventional procedure will be most effective.
Sources of Cancer Pain
The main sources include:
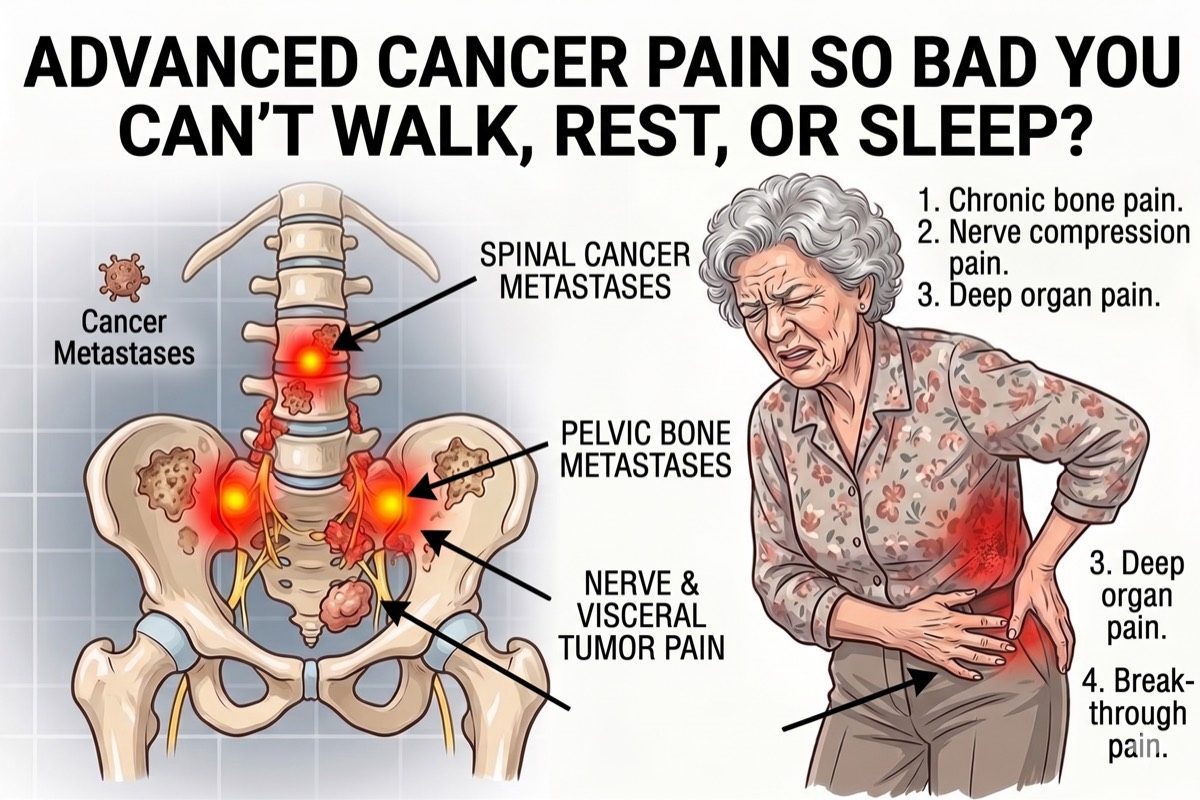
- Direct Tumour Invasion: Into bone, nerves, the spinal cord, or adjacent hollow organs. Produces a combination of nociceptive and neuropathic pain that may be severe.
- Vertebral Metastases: Bone destruction weakens vertebral bodies, causing pathological fractures that produce severe mechanical back pain and sometimes nerve compression.
- Visceral Involvement: Tumour invasion into the coeliac plexus (upper abdominal cancers) or hypogastric plexus (pelvic cancers) causes severe deep abdominal or pelvic pain that responds dramatically to targeted nerve destruction procedures such as Coeliac Plexus neurolysis or Splanchnic nerve RFA.
- Post-Surgical or Post-Radiotherapy Pain: Scar tissue, nerve damage from surgery, and radiation-induced fibrosis can cause persistent pain that continues after active cancer treatment.
- Chemotherapy-Induced Peripheral Neuropathy: Many chemotherapy agents cause painful burning, tingling, or numbness in the hands and feet that can persist after treatment ends.
Interventional vs Oral Medication Alone
Oral opioids are the backbone of cancer pain management and will always remain so. Interventional procedures complement the WHO Pain Ladder; they do not replace it.
Coeliac Plexus neurolysis and Splanchnic nerve RFA are among the most powerful options. In patients with pancreatic or upper abdominal cancer pain, these procedures can reduce pain scores by 50 to 70 percent and cut opioid requirements substantially. This directly reduces opioid-related constipation, sedation, and nausea.
Intrathecal drug delivery systems deliver morphine directly into the spinal fluid at doses as low as one-hundredth of what is needed orally, achieving better pain control with far fewer systemic side effects.
All decisions are made in close coordination with the patient's oncologist and palliative care team.
Assessment and Planning
Dr. Ashu Kumar Jain conducts a comprehensive cancer pain assessment before recommending any procedure, working as part of the multidisciplinary team.
- Detailed pain assessment: character, location, severity, temporal pattern, and impact on quality of life
- Review of oncology records, CT/PET/MRI imaging, and current medication
- Assessment of opioid responsiveness and side effect burden
- Neurological examination where neuropathic pain or nerve compression is suspected
- Discussion with the patient's oncologist and palliative care team before any interventional plan is finalised
Check If You Need This Treatment
What we offer?
Our approach to cancer pain management
We use targeted, minimally invasive procedures that complement your oncology treatment and go directly to the source of the pain.
-
 Stellate Ganglion RFA / Neurolysis: for head and neck cancer pain
Stellate Ganglion RFA / Neurolysis: for head and neck cancer pain
-
T2T3 Sympathectomy: for upper limb pain
-
Splanchnic RFA / Neurolysis: for pancreas, gall bladder, liver, and upper GI cancer pain
-
Lumbar Sympathectomy: for CRPS of lower limb (leg) pain
-
Superior Hypogastric Neurolysis: for pelvic cancer pain
-
Ganglion Impar RFA / Neurolysis: for perianal pain
-
Splanchnic Nerve RFA

Frequently asked questions
Will interventional procedures replace my current pain medication?
No. Interventional procedures work alongside your oral medication, not instead of it. In many cases they significantly reduce the dose of opioids needed to control pain, which also reduces side effects. Your overall pain management plan continues to be coordinated with your oncologist and palliative care team.
What is Coeliac Plexus neurolysis / Splanchnic nerve RFA and who is it for?
The coeliac plexus is a network of nerves in the upper abdomen that carries pain signals from the stomach, pancreas, liver, gallbladder, and small bowel. In patients with upper abdominal cancer, procedures such as Coeliac Plexus neurolysis (chemical destruction of the plexus) or Splanchnic nerve radiofrequency ablation (RFA) can reduce pain scores by 50 to 70 percent. These are particularly effective for pancreatic and other upper abdominal cancer pain.
What is intrathecal drug delivery?
An intrathecal drug delivery system (also called a pain pump) delivers very small doses of morphine or other analgesics directly into the spinal fluid surrounding the spinal cord. The drug acts at the spinal level before reaching the brain, achieving much stronger pain control at doses as low as one-hundredth of what is required orally. This dramatically reduces systemic side effects such as sedation and constipation.
Can vertebroplasty or kyphoplasty help with cancer bone pain?
Yes. When a vertebral body collapses due to a metastatic lesion, it causes severe mechanical back pain. Vertebroplasty stabilises the fracture by injecting bone cement into the collapsed vertebra. Kyphoplasty additionally restores some vertebral height. Both procedures provide rapid and often dramatic pain relief and improved function, usually within 24 to 48 hours.
At what stage of cancer should I consider an interventional pain consultation?
An interventional pain consultation is appropriate at any stage when pain is not adequately controlled by oral medication, when opioid side effects are limiting adequate dosing, or when pain is significantly affecting quality of life. Earlier referral tends to produce better outcomes. There is no need to wait until all oral options are exhausted.
Is interventional pain management safe for cancer patients?
Yes, with careful patient selection. Dr. Ashu Kumar Jain reviews all relevant oncology reports, bloodwork, and imaging before any procedure. Procedures are selected to match the patient's functional status and overall condition. For many cancer patients, the benefit in terms of pain reduction and opioid sparing far outweighs the procedural risk.
Any concern?