Shoulder Pain: Causes, Symptoms, and Treatment Options
Shoulder pain can make even simple tasks painful and limit how much you can move your arm. Most causes have a clear diagnosis and respond well to targeted interventional treatment.

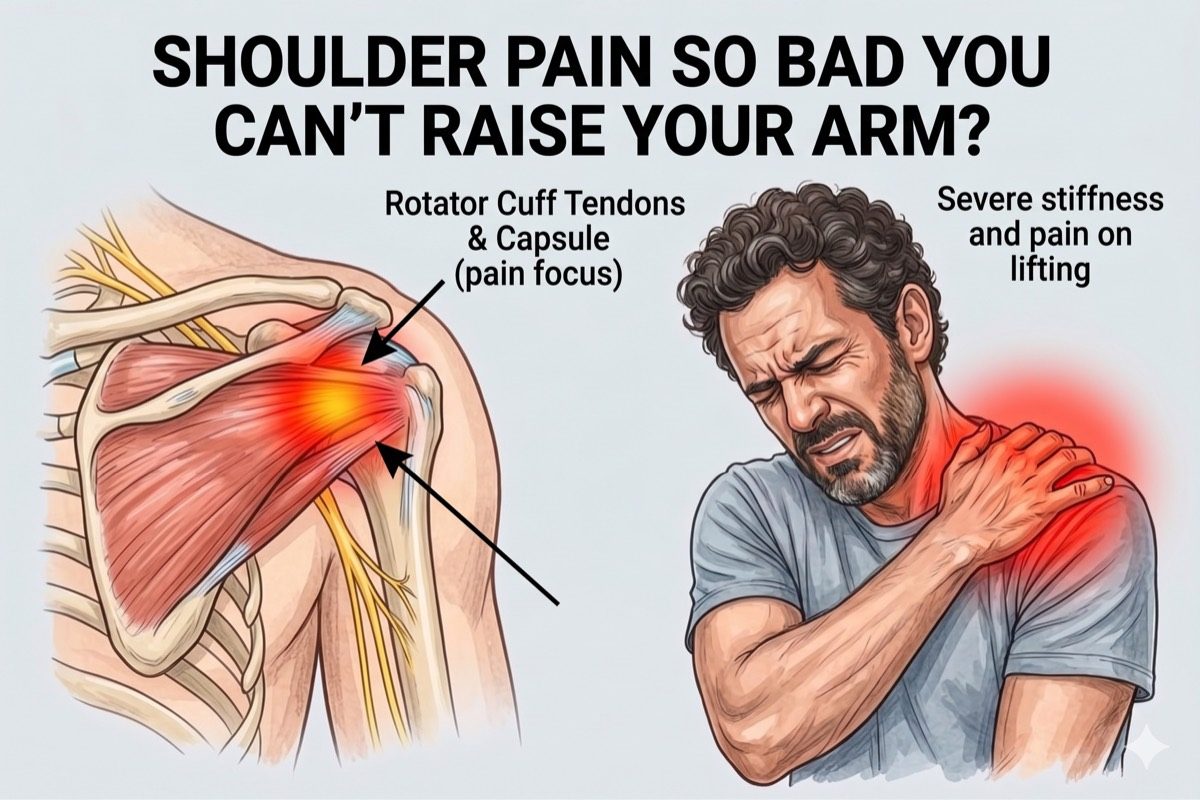
The shoulder is the most mobile joint in the body, which also makes it one of the most vulnerable to injury and pain. Problems can arise from the joint itself, the surrounding tendons, the bursa, or the nerves supplying the area.
What is Shoulder Pain?
Shoulder pain refers to any discomfort felt in or around the shoulder joint. It can range from a dull ache to sharp pain that worsens with movement or at night when lying on the affected side.
The shoulder joint is surrounded by four rotator cuff muscles, a fluid-filled bursa, and is supported by the acromioclavicular (AC) joint above. Each of these can independently become a source of pain.
Many shoulder conditions are treatable without surgery. An accurate diagnosis guides the selection of the most effective procedure.

Symptoms of Shoulder Pain
Common symptoms include:
If shoulder pain is severe, has lasted more than 4 weeks, or comes with significant weakness or loss of movement, you should see a specialist promptly.
- Pain in the shoulder that may radiate down the upper arm
- Reduced ability to raise the arm or reach overhead
- Stiffness that makes it hard to rotate or extend the arm
- Pain at night, particularly when lying on the affected side
- A catching or clicking sensation during shoulder movement
- Weakness when lifting or carrying objects
- Swelling or tenderness at the front of the shoulder
What Causes Shoulder Pain?
Shoulder pain can come from several different structures. The most common causes are:
Risk factors include repetitive overhead work or sport, prior shoulder injury, age over 45, diabetes (a strong risk factor for frozen shoulder), and prolonged immobility.
- Rotator Cuff Tendinopathy or Tear: The rotator cuff tendons become inflamed or partially torn from repetitive use or injury, causing pain with overhead activities and weakness.
- Subacromial Bursitis: The bursa between the rotator cuff and the acromion becomes inflamed, causing sharp pain when raising the arm to the side or overhead.
- Frozen Shoulder (Adhesive Capsulitis): The shoulder joint capsule thickens and tightens, severely limiting all movements and causing significant pain, especially at night.
- Acromioclavicular Joint Arthritis: The AC joint at the top of the shoulder degenerates and causes pain with reaching across the body or lifting overhead.
- Glenohumeral Osteoarthritis: Wear and tear within the main ball-and-socket joint causes deep, aching pain and progressive stiffness.
Frozen Shoulder (Adhesive Capsulitis)
Frozen shoulder is one of the most disabling shoulder conditions. It develops when the capsule surrounding the shoulder joint becomes inflamed and scarred, restricting movement in all directions. Even passive movements performed by a therapist become painful and very limited.
It typically progresses through three stages: a painful freezing stage, a stiffening stage with severe restriction, and a gradual thawing stage. Without treatment, the thawing stage can take 12 to 24 months to complete.
Hydrodilatation, a procedure that uses guided injection of fluid to expand and stretch the joint capsule, can significantly accelerate recovery and reduce pain when performed at the right stage of the condition.
How is Shoulder Pain Diagnosed?
Diagnosis begins with a clinical examination that assesses range of motion, strength, and the specific pattern of pain. Dr. Ashu Kumar Jain examines both active and passive movement to distinguish between different shoulder conditions before recommending any imaging.
- Clinical examination including range of motion, strength testing, and impingement tests
- MRI of the shoulder to assess the rotator cuff, bursa, and joint cartilage
- Ultrasound for real-time assessment of tendons and bursae during movement
- X-rays to check joint space, bone spurs, and AC joint changes
- Diagnostic suprascapular nerve block or intra-articular injection to confirm the pain source
Check If You Need This Treatment
I have persistent shoulder or upper arm pain
I have MRI or ultrasound showing a tear, bursitis, or capsule thickening
Pain has lasted more than 4 to 6 weeks
Pain limits my daily activities or sleep
Conservative treatments haven’t fully helped
What we offer?
Our approach to treating shoulder pain
We use targeted, minimally invasive procedures that go directly to the source of the pain.
 Suprascapular Nerve Block for rapid, sustained relief from shoulder joint and rotator cuff pain
Suprascapular Nerve Block for rapid, sustained relief from shoulder joint and rotator cuff pain- Intra-articular Corticosteroid Injection to reduce inflammation inside the shoulder joint
- Hydrodilatation for frozen shoulder, guided capsule expansion to restore movement
- Acromioclavicular (AC) Joint Injection for targeted relief of AC joint arthritis
- Ultrasound Guided PRP (Platelet Rich Plasma) regenerative therapy to treat tendinosis and tendinitis
- Pulsed RFA of the Suprascapular Nerve for prolonged relief from shoulder pain
- Cooled RFA of the Shoulder Joint for prolonged pain relief in severe glenohumeral osteoarthritis where joint replacement is not an option

Frequently asked questions
What are the most common causes of shoulder pain?
The most common causes are rotator cuff tendinopathy, subacromial bursitis, frozen shoulder, and AC joint arthritis. These conditions are often distinguishable on clinical examination, and an MRI or ultrasound confirms the diagnosis. Each condition has a different treatment approach.
How is frozen shoulder different from a rotator cuff problem?
Frozen shoulder restricts all movements of the shoulder, including passive movements where someone else moves your arm for you. A rotator cuff problem typically limits active movements more than passive ones, and the restriction is directional rather than global. The distinction matters because the treatments are quite different.
What interventional treatments are available for shoulder pain?
We offer suprascapular nerve blocks for broad shoulder pain relief, intra-articular injections for joint inflammation, hydrodilatation for frozen shoulder, and AC joint injections for acromioclavicular arthritis. The right procedure depends on the confirmed diagnosis.
What is hydrodilatation and how does it help frozen shoulder?
Hydrodilatation is an image-guided procedure where a mixture of saline, local anaesthetic, and corticosteroid is injected into the shoulder joint under pressure. This expands the contracted capsule, reduces inflammation, and helps restore range of motion. It is most effective during the freezing and frozen stages of adhesive capsulitis.
Will I need surgery for a rotator cuff tear?
Not necessarily. Many partial rotator cuff tears respond well to a combination of interventional injections and a structured rehabilitation programme. Surgery is considered when the tear is large, full-thickness, or when pain and weakness persist despite thorough non-surgical treatment.
How long does shoulder pain typically last?
This depends significantly on the cause. Bursitis often improves within 6 to 12 weeks with the right treatment. Frozen shoulder without treatment can persist for 1 to 3 years. With interventional procedures and guided rehabilitation, most patients see meaningful improvement within weeks to a few months.
When should I see a specialist for shoulder pain?
See a specialist if your shoulder pain has lasted more than 4 weeks, is worsening, interferes with sleep, or is associated with significant weakness or loss of movement. Early treatment of frozen shoulder in particular produces much better outcomes than waiting.
What is the role of PRP (Platelet Rich Plasma) in treating shoulder pain?
PRP is a regenerative therapy that uses a concentrated preparation of your own platelets to stimulate healing in damaged tendons and muscles. In shoulder pain, ultrasound guided PRP is used to treat tendinosis and partial rotator cuff tears. It promotes tissue repair and can significantly reduce pain and improve function, often avoiding the need for surgery.
Should I take blind corticosteroid injections in the shoulder?
Absolutely not. Blind corticosteroid injections given without imaging guidance carry a serious risk of being injected directly into a tendon rather than the joint or bursa. This can cause complete tendon or muscle rupture and permanent deformity. All corticosteroid injections for the shoulder must be given under ultrasound guidance to ensure precise placement and safety.
Do all rotator cuff muscle tears require surgery?
No. If the tear involves less than 50% of the tendon thickness, targeted PRP therapy delivered under ultrasound guidance can stimulate healing, restore tendon integrity, and help you avoid surgery altogether. Surgery is generally reserved for large full-thickness tears that do not respond to non-surgical treatment.
How many sessions of PRP therapy are needed for shoulder pain?
Typically three to five sessions are required. Each session is spaced four weeks apart to allow the platelets to complete their regenerative cycle before the next dose is administered.
What is the success rate of PRP therapy for shoulder pain?
Reported success rates for ultrasound guided PRP in shoulder tendinopathy and partial tears are around 70%. Results depend on the size of the tear, the stage of the condition, and compliance with the full course of treatment.
Can PRP therapy temporarily increase my shoulder pain?
Yes, a temporary increase in pain is possible during the first or second session. This is a normal part of the healing response as the platelets begin stimulating tissue repair. The discomfort is usually mild to moderate and can be managed with a simple analgesic such as paracetamol.
Can I take steroids or anti-inflammatory medications while undergoing PRP therapy?
No. Corticosteroids and non-steroidal anti-inflammatory drugs (NSAIDs) suppress the very healing response that PRP depends on. Taking them alongside PRP therapy will significantly reduce its effectiveness and can cause the treatment to fail. All such medications must be stopped at least four weeks before beginning PRP therapy.
Can PRP injections be given without imaging guidance?
Absolutely not. For PRP to be effective, the platelets must be delivered precisely to the site of tendinitis or the muscle tear under ultrasound guidance. A blind injection misses the target and provides no benefit. Image guidance is non-negotiable for PRP therapy in the shoulder.