Spine surgery is a major, irreversible procedure. It has genuine indications - situations where it is the right and necessary choice. But it also has a long history of being offered too early, before less invasive treatments have been given a proper trial. Epidural steroid injections occupy the space between painkillers and the operating theatre, and for many patients, that space is exactly where they need to spend more time.
What Does an Epidural Steroid Injection Actually Do?
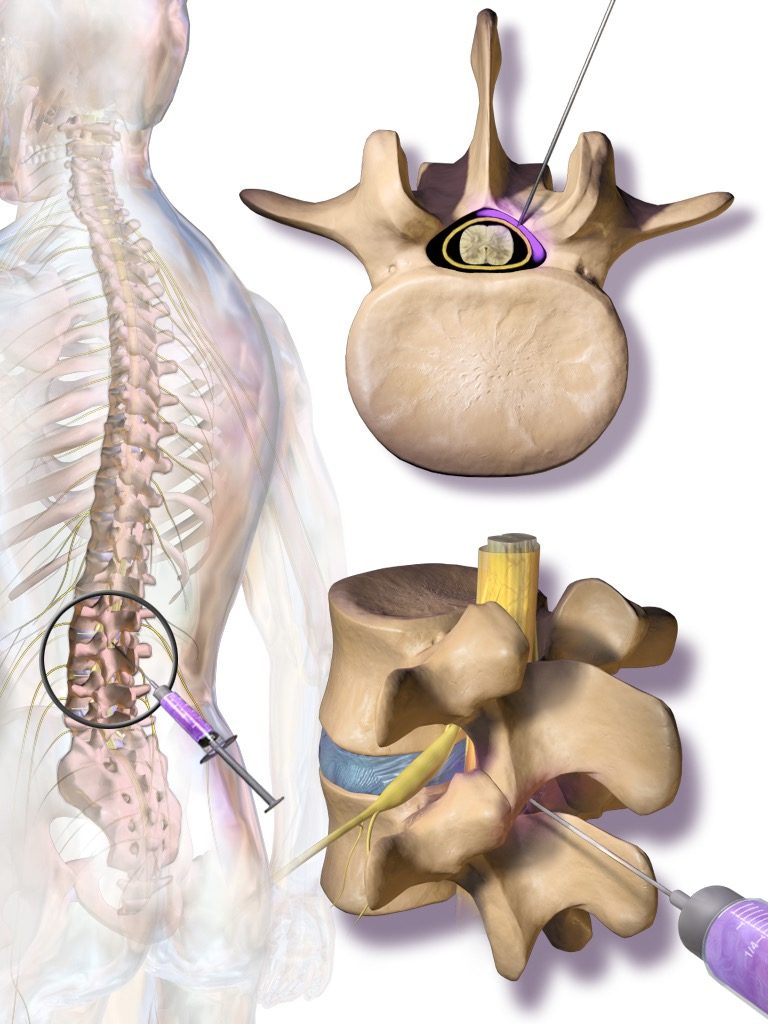
An epidural steroid injection (ESI) delivers a combination of corticosteroid and local anaesthetic directly into the epidural space - the area surrounding the spinal nerves. For pain caused by nerve compression (a herniated disc pressing on a nerve root, or narrowed spinal canal in stenosis), the injection reduces the inflammation around the nerve, relieves the swelling, and often interrupts the pain cycle significantly enough for the patient to rehabilitate and recover.
It is a targeted, anti-inflammatory treatment. It does not repair a disc. What it does is create a window of reduced pain - a window that, for many patients, is wide enough that surgery becomes unnecessary.
When Is an ESI the Right Choice?
ESI is most effective when the primary problem is nerve inflammation, not structural instability. The ideal candidates include patients with:
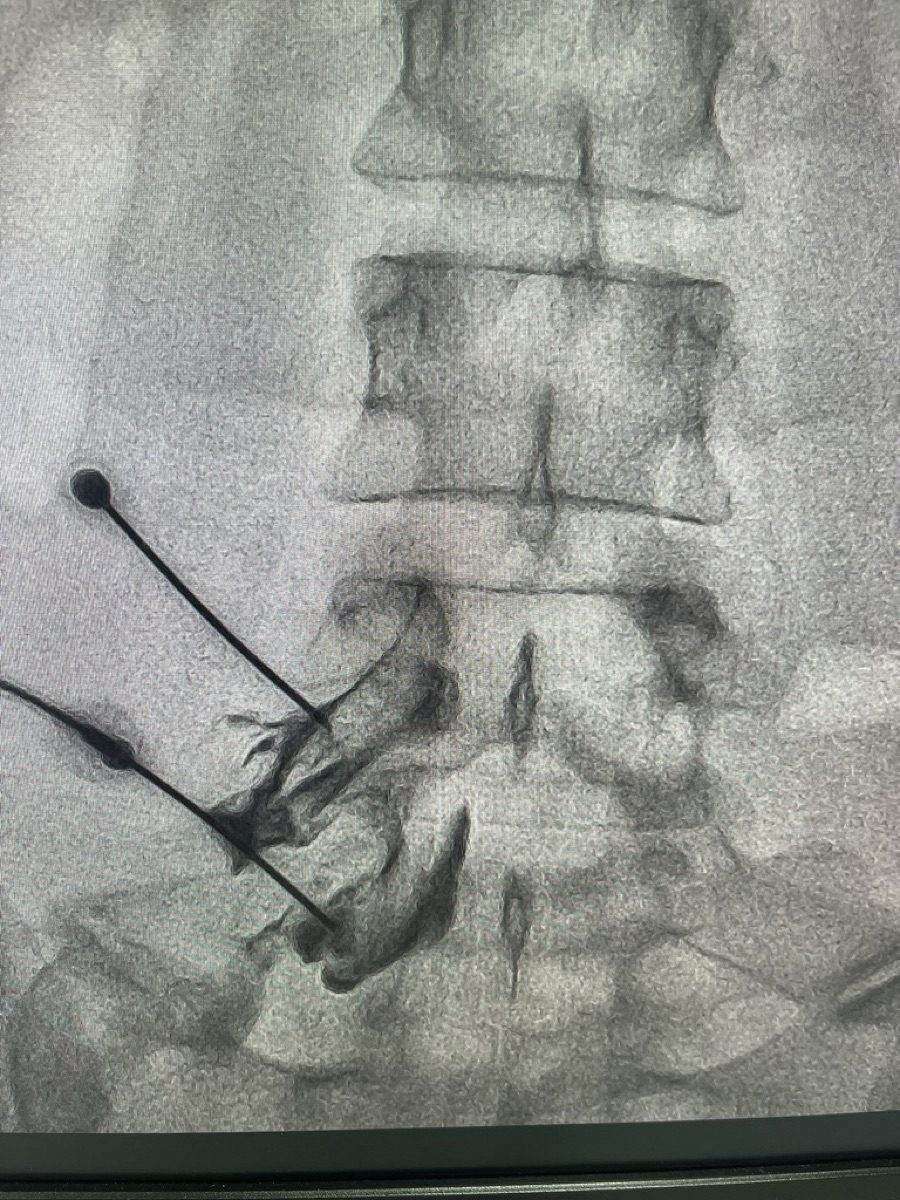
In these scenarios, a well-placed ESI - delivered under fluoroscopic guidance to the correct level and side - can produce dramatic relief. Multiple injections, spaced weeks apart, may be needed for sustained benefit.
- Acute or subacute sciatica from a herniated disc (especially within the first 3–6 months)
- Spinal stenosis causing leg pain (neurogenic claudication), particularly in older patients
- Radiculopathy - nerve root pain, numbness, or burning that radiates down an arm or leg
- Post-surgical pain where residual nerve inflammation persists after an earlier procedure
When Is Surgery the Right Choice?
Surgery is clearly indicated in specific, well-defined situations:
- Cauda equina syndrome - compression of the nerves at the base of the spine causing loss of bladder or bowel control. This is a surgical emergency.
- Progressive neurological deficit - new or worsening weakness in the leg or arm that is not responding to conservative treatment.
- Structural instability - spinal instability (spondylolisthesis) causing debilitating symptoms that cannot be managed non-surgically.
- Failed conservative management - a patient who has genuinely completed a full course of physiotherapy and a series of appropriately placed epidural injections without adequate relief.
"Surgery addresses structure. Injections address inflammation. In most cases of disc-related nerve pain, the inflammation is the primary driver - and injections address it far more directly than a scalpel can."
What the Research Shows
Multiple large, well-designed clinical trials have compared ESI with surgery for lumbar disc herniation. The consistent finding: at one year, outcomes are similar between patients who had ESI and those who had surgery. The surgical patients often improved faster in the first few weeks, but by 12 months, the groups converged.
Critically, a significant proportion of patients initially assigned to surgery avoided it altogether after receiving ESI - their symptoms resolved sufficiently that surgery was no longer needed. Surgery, once performed, changes spinal anatomy permanently and may create its own long-term problems (adjacent segment disease, scar tissue formation around nerves).
At Jain Pain Clinic, Dr. Ashu Kumar Jain reviews each patient's imaging and clinical history carefully before recommending any route, ensuring a properly placed and correctly sequenced course of ESI has been completed before a surgical referral is considered.
The Practical Takeaway
If you have been told you need spine surgery and you have not yet had a consultation with an interventional pain specialist, that consultation is worth having. The question to ask is not "surgery or no surgery" - it is "have I exhausted all reasonable options short of surgery?"
An ESI is a same-day procedure with minimal downtime and far lower risk than surgery. If it works, it may resolve your problem completely. If it does not provide sufficient relief after a proper trial, you have lost nothing - and surgery remains available with even clearer indication.
Dr. Ashu Kumar Jain at Jain Pain Clinic in Gurugram performs fluoroscopy-guided epidural steroid injections for disc herniation, spinal stenosis, and radiculopathy. If you have been advised surgery and want to explore whether an ESI is appropriate first, book a consultation.