Spinal Cord Injury Pain: Types, Causes, and Interventional Treatment
Pain after a spinal cord injury is common, complex, and undertreated. It is not simply a consequence to accept. With interventional pain management, the right combination of procedures can restore comfort and support rehabilitation.
More than two thirds of people living with a spinal cord injury experience significant pain. This pain is often more debilitating than the paralysis itself. It interferes with sleep, rehabilitation, and quality of life. Targeted interventional treatment offers real hope for control.
Understanding Pain After Spinal Cord Injury
Not all pain after a spinal cord injury (SCI) is the same. Understanding the type of pain is essential for choosing the right treatment.
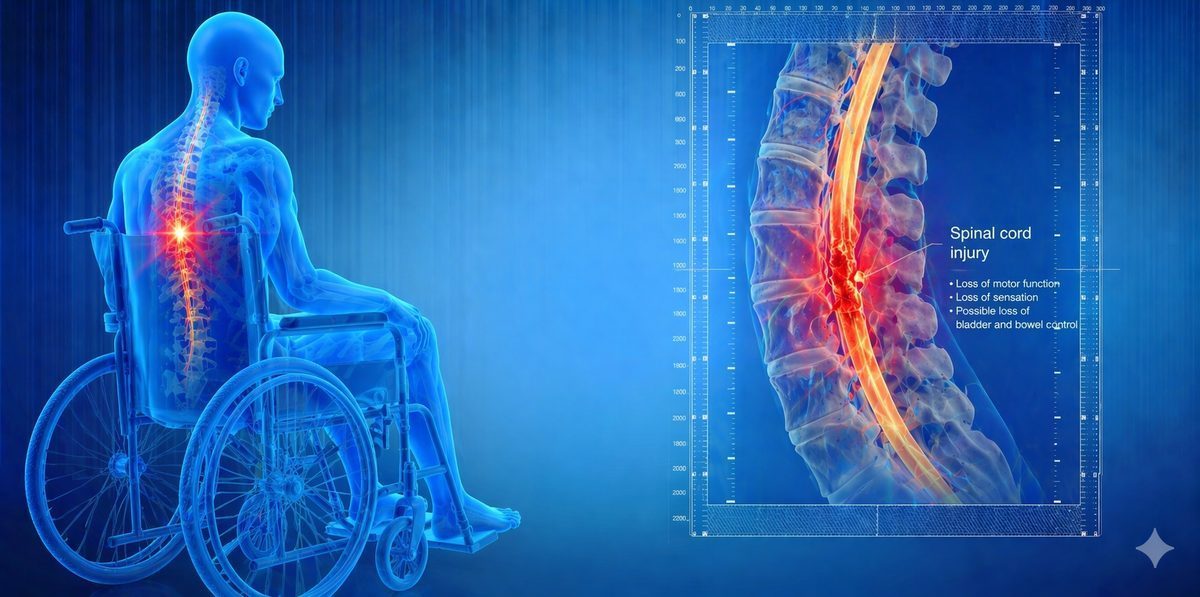
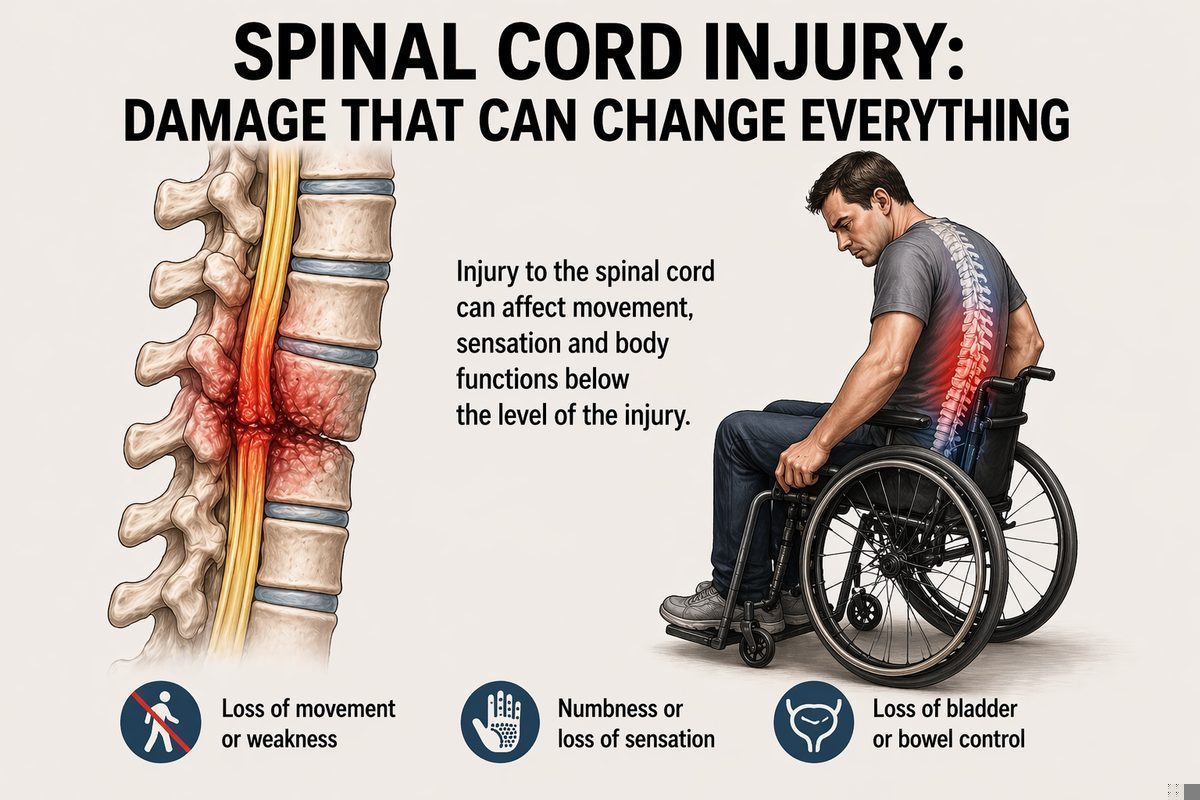
Neuropathic pain at and below the injury level is the most common type. It is caused by damage to the spinal cord itself. The nervous system generates abnormal signals and interprets them as burning, stabbing, or electric pain, even in areas where sensation is otherwise reduced or absent. This is one of the most difficult types of pain to treat with medications alone.
Musculoskeletal pain above the injury level is very common in wheelchair users. The shoulders, neck, and upper back take on enormous strain during transfers and manual wheelchair propulsion. Over time, this causes rotator cuff damage, cervical joint degeneration, and significant chronic pain.
Spasticity-related pain occurs when abnormal spinal cord signalling causes involuntary muscle spasms. These spasms can be extremely painful. They may also cause joint contractures over time, which adds further musculoskeletal pain to the picture.
Visceral pain felt in the abdomen or pelvis is less common but deeply unpleasant. It is caused by disrupted autonomic nerve supply to the internal organs.

Symptoms of SCI Pain
The symptoms vary depending on the type of pain and the level of the injury.
Pain that is worsening or changing in character should always be assessed promptly. New or escalating pain after SCI can sometimes indicate a correctable cause such as a pressure ulcer, urinary tract infection, or autonomic dysreflexia.
- Burning, stabbing, or electric-shock like pain in or below the level of injury
- Constant aching or pressure pain in the trunk or limbs
- Painful muscle spasms that wake the patient from sleep
- Sharp shoulder, neck, or upper back pain from overuse
- Allodynia, which is pain triggered by a light touch or change in temperature in areas of reduced sensation
- Abdominal cramping or pelvic pain with no clear cause
- Pain that worsens with bladder or bowel issues, pressure sores, or infections
Why is SCI Pain So Difficult to Treat?
Several reasons make SCI pain particularly challenging.
- Central Sensitisation: The injured spinal cord itself becomes hyperexcitable. Neurons fire spontaneously and amplify incoming signals. This is driven by structural and chemical changes in the cord that persist long after the original injury.
- Loss of Inhibitory Control: The brain normally sends descending signals that moderate pain processing in the spinal cord. After SCI, these inhibitory signals can no longer reach below the injury level. Pain is processed without its normal brakes.
- Neuroplasticity: The nervous system rewires itself after injury. Some of this rewiring is helpful for recovery. Other changes unfortunately create new pain circuits that were not present before the injury.
- Multiple Overlapping Pain Types: Most SCI patients have neuropathic pain, musculoskeletal pain, and spasticity all at once. Each type needs a different approach, which makes treatment more complex.
- Undertreatment: Healthcare providers sometimes focus entirely on rehabilitation and mobility and overlook the significant pain burden. This delays effective pain management and allows central sensitisation to become more entrenched.
What Conditions Worsen SCI Pain?
Certain factors can trigger or amplify pain in SCI patients. These are sometimes called nociceptive triggers.
Identifying and correcting these triggers is always the first step. It can significantly reduce pain without any invasive treatment.
- Urinary tract infections or bladder distension
- Constipation and bowel distension
- Pressure ulcers or skin breakdown
- Deep vein thrombosis
- Autonomic dysreflexia (a sudden dangerous rise in blood pressure triggered by a stimulus below the injury)
- Poor posture, ill-fitting wheelchair, or prosthetic equipment
- Anxiety, depression, and poor sleep
How is SCI Pain Assessed?
A thorough, systematic assessment is essential before treatment is planned.
- Full neurological assessment including the level and completeness of the SCI using standard classification tools
- Pain mapping to identify which areas are affected and what type of pain is present in each area
- MRI of the spine to check for syrinx (fluid-filled cavities in the cord), tethering, or hardware complications in surgical patients
- Assessment of spasticity severity using clinical scales
- Urodynamic studies and bowel function assessment to rule out visceral triggers
- Psychological assessment, since depression and anxiety are common after SCI and significantly amplify pain perception
Check If You Need This Treatment
I have burning, stabbing, or electric pain at or below my injury level
I have painful muscle spasms or spasticity that affect my daily life
Pain is limiting my ability to take part in rehabilitation or daily activities
Pain has been present for more than one month following my injury
Oral medications have not provided adequate relief
What we offer?
Our approach to treating spinal cord injury pain
We use a carefully planned combination of interventional procedures to address neuropathic pain, spasticity, and musculoskeletal pain arising from life with a spinal cord injury.
 Spinal Cord Stimulation (SCS) to modulate central pain processing and reduce burning neuropathic pain at and below the injury level, particularly effective for incomplete SCI
Spinal Cord Stimulation (SCS) to modulate central pain processing and reduce burning neuropathic pain at and below the injury level, particularly effective for incomplete SCI- Intrathecal Drug Delivery (Pain Pump) to deliver medication directly into the spinal fluid, achieving powerful pain and spasticity control with a fraction of the oral dose, reducing systemic side effects greatly
- Epidural Steroid Injection for musculoskeletal pain components such as cervical or thoracic radiculopathy arising from adjacent segment degeneration above the SCI level
- Botulinum Toxin Injection for Spasticity to reduce painful muscle overactivity, improve posture, ease personal care, and reduce spasm-related pain
- Shoulder and Rotator Cuff Injection or RFA for pain arising from repetitive strain in manual wheelchair users and during transfers
- Sympathetic Nerve Block to address visceral or autonomic pain components, particularly relevant in high thoracic and cervical injuries
Frequently asked questions
Can a person with no sensation below the injury still feel pain there?
Yes. This is one of the most confusing aspects of SCI pain. It is possible to have both markedly reduced sensation and severe pain in the same area. The pain is generated centrally by the injured spinal cord and the brain. It does not require an intact sensory pathway to be perceived. This type of pain is called central neuropathic pain and it is a recognised condition. It is not imagined and should be managed actively.
What is an intrathecal pump and how does it help in SCI?
An intrathecal pump is a small device implanted under the skin of the abdomen. It delivers medication directly into the spinal fluid through a small catheter. This bypasses the blood-brain barrier, which means very small doses achieve a much stronger effect than the same medication taken orally. It is particularly valuable in SCI for managing both severe neuropathic pain and spasticity. Baclofen delivered intrathecally can dramatically reduce violent painful spasms. The dose can be adjusted non-invasively using a programmer. Side effects are significantly lower than with high-dose oral medication.
Is spinal cord stimulation safe in someone who already has a spinal cord injury?
In many patients with incomplete SCI, spinal cord stimulation is a well-established and safe option. A pre-procedure MRI review and careful patient selection are essential. The electrode is placed above the level of injury to stimulate the intact cord. This modulates the pain signals travelling through the cord to the brain. It carries a good safety record and significant evidence for benefit in this group. Suitability is assessed individually during consultation.
Why do my shoulders hurt so much when my injury is in my spine?
Shoulder pain is one of the most common sources of pain above the injury level in SCI patients who use wheelchairs. Manual wheelchair propulsion, transfers, and pressure relief movements place enormous repetitive stress on the shoulder joint and rotator cuff. Studies show that over 60% of long-term manual wheelchair users develop significant shoulder pathology. This is pure musculoskeletal pain, entirely separate from neuropathic SCI pain, and it responds very well to targeted injections, physiotherapy, and if needed, radiofrequency procedures.
Will treating my pain affect my rehabilitation?
Good pain control generally improves rehabilitation outcomes, not reduces them. Pain is one of the single biggest barriers to participation in physiotherapy and occupational therapy. Patients who sleep better, have fewer spasms, and can engage more fully in rehab sessions make faster progress. Treating spasticity pain also often reveals underlying motor function that was masked by the spasms. Pain management and rehabilitation are not competing tools. They work best together.
How soon after my spinal cord injury should I see a pain specialist?
Early assessment is beneficial, even within the first weeks after injury. Pain that is not addressed early tends to become more entrenched due to central sensitisation. A pain specialist working alongside the rehabilitation team can significantly reduce the intensity and chronicity of SCI pain. If you are already living with chronic SCI pain, it is never too late to seek a specialist assessment. Effective treatments are available regardless of how long the pain has been present.