Knee osteoarthritis is one of the most prevalent causes of disability in adults over 50. For patients with moderate to severe joint changes who have failed conservative management, knee replacement is a proven, effective treatment. The problem is not the surgery itself - it is that it is being offered far too early, to patients who would benefit enormously from less invasive interventional options that are rarely discussed with them.
Understanding Knee Pain: Not Always What It Appears
The knee joint is supplied by several sensory nerves - primarily the genicular nerves, branches of the femoral and common peroneal nerves. These nerves transmit pain signals from the joint capsule, ligaments, and periosteum. In osteoarthritis, even when cartilage loss is visible on X-ray, the severity of pain does not reliably correlate with the degree of structural damage seen on imaging.
This is a fundamental insight: two patients with identical X-ray findings may have wildly different pain experiences. One reason is that pain in knee osteoarthritis is substantially driven by sensitisation of these genicular nerves - which means targeting the nerves, rather than replacing the joint, can provide dramatic relief even without altering the underlying arthritis.
The Non-Surgical Toolkit for Knee Osteoarthritis
Intraarticular Injections
Corticosteroid injections directly into the knee joint reduce synovial inflammation and provide meaningful short-term relief for the majority of patients. Hyaluronic acid (viscosupplementation) injections are an alternative with a somewhat different mechanism - replacing the lubricating fluid the joint produces less of as it ages. These are appropriate early-stage options for patients with inflammatory flares or mild-moderate disease.
PRP (Platelet-Rich Plasma)
Autologous PRP injections - using concentrated growth factors from your own blood - have shown promising results in moderate knee osteoarthritis, reducing both pain and inflammation and potentially slowing joint degeneration. They are particularly useful for younger, active patients who want to delay any surgical intervention.
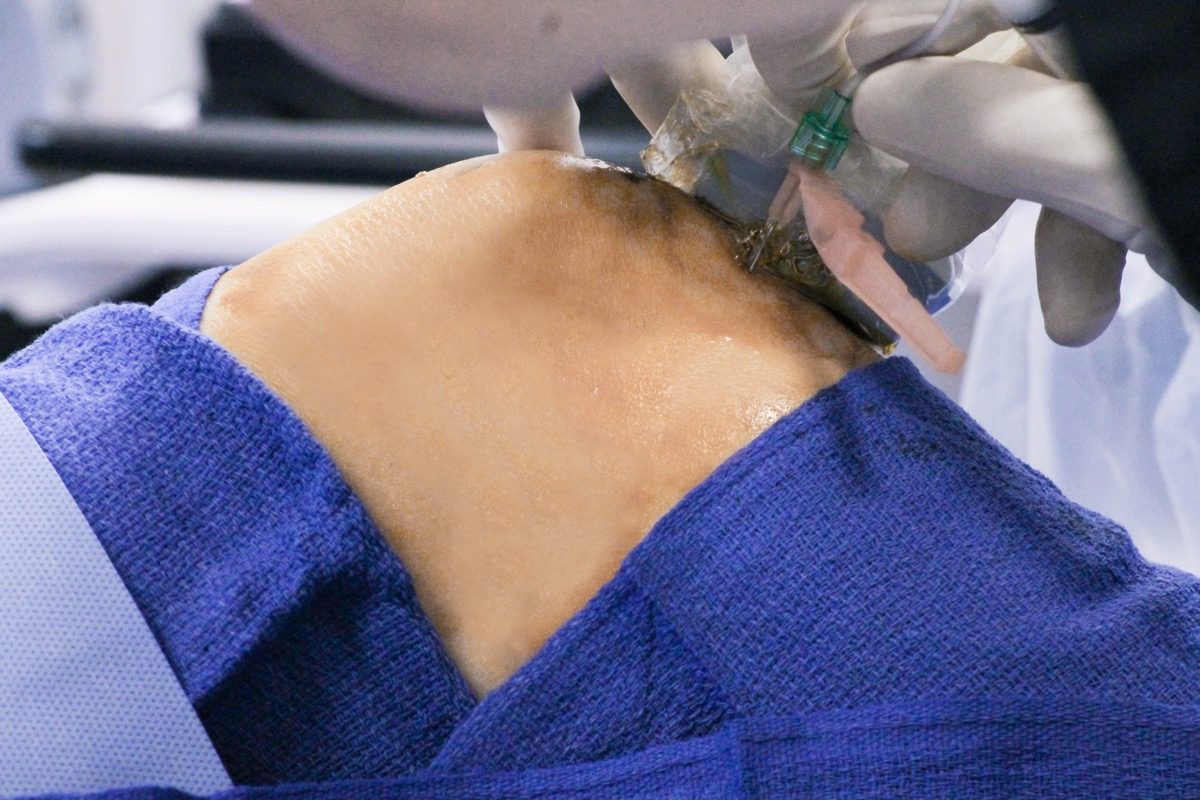
Genicular Nerve Block
A genicular nerve block involves injecting local anaesthetic around the three principal genicular nerves supplying the knee under ultrasound or fluoroscopic guidance. When the block produces significant pain relief - confirming that these nerves are the primary pain pathway - it opens the door to a more durable treatment: genicular nerve cooled radiofrequency ablation.
At Jain Pain Clinic in Gurugram, Dr. Ashu Kumar Jain performs genicular nerve blocks under image guidance. A strong response to the diagnostic block is the criterion used to confirm that a patient is a suitable candidate for cooled RFA, ensuring the ablation targets the right nerves.
Cooled Radiofrequency Ablation: The Breakthrough for Knee Pain
Cooled RFA is a significant advancement over conventional RFA for knee pain. Standard RF probes generate a small sphere of heat at the needle tip. Cooled RFA circulates water through the probe tip while generating the RF current - this cooling effect creates a larger ablation zone, more effectively covering the complex curved anatomy of the genicular nerves.
Clinical trial data shows that knee cooled RFA produces pain relief lasting 6 to 24 months or beyond in the majority of patients with knee osteoarthritis. Crucially, it achieves this without altering joint anatomy, without recovery time, and without the risks of general anaesthesia and major surgery.
"For patients who are medically unfit for surgery, or who are not yet ready for a knee replacement, cooled RFA changes the equation entirely. It is not a temporary fix - it is a legitimate long-term treatment for a condition that was previously managed only with escalating pain medication or surgery."
When Knee Replacement IS the Right Answer
It is important to be clear: knee replacement is a highly effective procedure with appropriate indications. It is the right choice when:
What is not appropriate is offering knee replacement as a first or early second treatment for patients with moderate osteoarthritis who have not had a proper trial of interventional options.
- Structural damage is severe enough that the joint mechanics are fundamentally compromised - significant varus or valgus deformity, bone-on-bone with collapse of normal joint space
- Multiple non-surgical treatments have been systematically tried and failed
- The patient's functional goals - returning to high-impact activities, for example - cannot be achieved with pain management alone
- The patient is medically fit for surgery and understands the recovery involved
The Practical Path Forward
If you have knee pain that is limiting your activities - difficulty walking distances, pain on stairs, night pain disrupting sleep - a consultation with an interventional pain specialist is the appropriate next step before any surgical conversation. The treatment options available are more sophisticated and more durable than most patients are told, and the risk-benefit calculation very often favours trying them first.
In many cases, a targeted programme of intraarticular injections followed by cooled RFA can restore meaningful function and quality of life for two or more years at a time - while keeping all future surgical options completely open.
Dr. Ashu Kumar Jain at Jain Pain Clinic, Gurugram, performs genicular nerve blocks and cooled radiofrequency ablation for knee osteoarthritis. If knee pain is limiting your daily life and you have been offered surgery as the only option, a specialist consultation is worth taking before committing to an operation.