Sciatica is one of the most common reasons patients visit a pain clinic - and one of the most commonly mismanaged conditions in general practice. The combination of low back pain and a shooting sensation down the leg is unmistakable, yet patients are routinely told to "give it time." Sometimes that advice is correct. Often, it costs them months of avoidable disability.
What Sciatica Actually Is
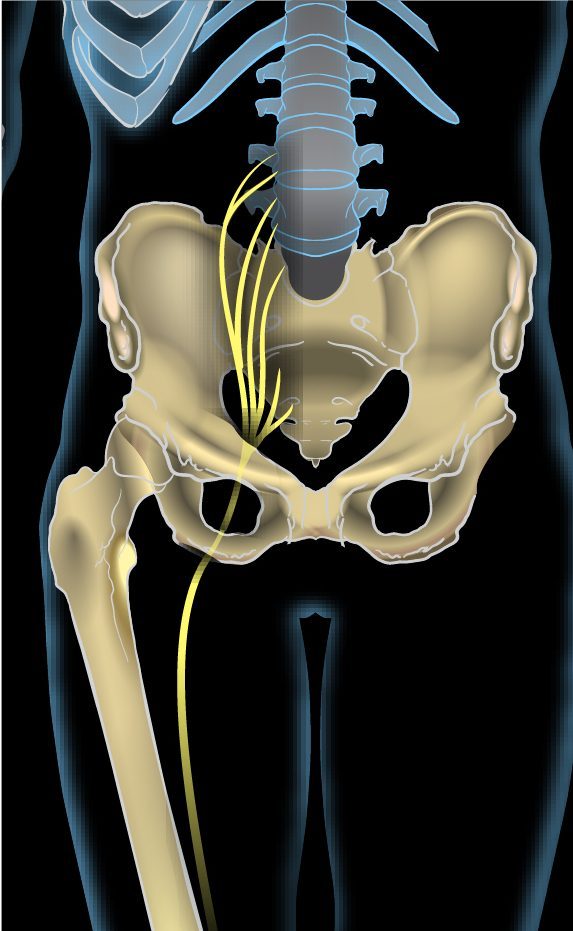
Sciatica is not a diagnosis - it is a symptom. It describes pain that originates in the lower back and radiates along the course of the sciatic nerve: through the buttock, down the back of the thigh, and into the calf or foot. The pain is typically described as sharp, burning, or electric - quite different from the dull ache of muscle strain.
The cause is almost always nerve root compression. A herniated lumbar disc is the most common culprit - the soft nucleus of a disc bulges through its outer casing and presses against an adjacent nerve root. Spinal stenosis (narrowing of the spinal canal) is the second most common cause, particularly in patients over 60. Less commonly, a piriformis muscle spasm can compress the sciatic nerve without any disc involvement.
Understanding this distinction matters because the treatment approach depends entirely on the cause. A herniated disc causing sciatica responds differently to treatment than stenosis-related sciatica.

The Problem with Waiting
A significant proportion of acute sciatica from disc herniation does improve with time. Studies suggest roughly 50 to 60 percent of patients have meaningful improvement within 6 to 12 weeks. This is the basis for the "wait and see" advice. But the numbers cut the other way as well: 40 to 50 percent do not improve significantly without targeted treatment.
The deeper problem with prolonged waiting is that persistent nerve compression leads to progressive nerve damage. What begins as reversible inflammation can, over months, cause permanent changes in nerve function - areas of lasting numbness, chronic weakness, or long-term changes in how the nervous system processes pain signals. The window for the most effective intervention is typically the first three to four months.
Warning Signs That Require Immediate Attention
While most sciatica is painful but not dangerous, certain features indicate an urgent or emergency situation:
If any of these features are present, do not wait for a scheduled appointment. Attend an emergency department immediately.
- Loss of bladder or bowel control - this is cauda equina syndrome, a surgical emergency requiring immediate hospital assessment.
- New progressive weakness in the leg - difficulty lifting the foot (foot drop), or rapidly weakening leg muscles, indicates significant nerve compromise and needs urgent evaluation.
- Bilateral leg symptoms - pain, weakness, or numbness affecting both legs simultaneously suggests central canal involvement and warrants urgent imaging.
- Saddle anaesthesia - numbness in the inner thighs and perineal area is another feature of cauda equina syndrome.
"Most sciatica is mechanical and responds excellently to targeted interventional treatment. The patients who do worst are those who wait so long that the nerve has been compressed for many months - early, precise treatment produces far better outcomes."
Why Physiotherapy Alone Often Falls Short
Physiotherapy is a valuable part of sciatica management - particularly for long-term rehabilitation, core strengthening, and prevention of recurrence. Where it is insufficient is in the acute phase when active nerve compression is generating severe pain.
An inflamed, compressed nerve root does not benefit significantly from exercise when it is in a state of acute biochemical irritation. Anti-inflammatory treatment - delivered as close to the nerve as possible - is what creates the conditions in which physiotherapy can then do its work effectively.
What an Epidural Steroid Injection Does for Sciatica
A transforaminal epidural steroid injection places corticosteroid and local anaesthetic directly at the affected nerve root - the precise location where inflammation is occurring. This is far more targeted than oral anti-inflammatory medication, which reaches every tissue in the body at low concentration, rather than the exact nerve root at therapeutic concentration.
The corticosteroid reduces swelling around the compressed nerve root, breaking the inflammatory cycle that sustains sciatica pain. Many patients experience significant relief within days to two weeks. For those with disc herniation, this window of reduced pain allows the disc to heal and decompression to occur naturally, often making surgery unnecessary.
At Jain Pain Clinic in Gurugram, Dr. Ashu Kumar Jain performs transforaminal epidural steroid injections under live fluoroscopic guidance, targeting the precise nerve root level and side identified on the patient's MRI - not a generalised injection, but a placement matched to the specific structural finding.
Other Interventional Options for Sciatica
When epidural steroid injections provide incomplete or short-lived relief, other targeted interventions include:
Dr. Ashu Kumar Jain at Jain Pain Clinic in Gurugram specialises in the full range of interventional treatments for sciatica, from transforaminal epidural steroid injections to pulsed RFA and biacuplasty. If sciatica has been limiting your mobility for more than six weeks, a specialist assessment can identify the right treatment and prevent longer-term nerve damage.
- Pulsed radiofrequency treatment of the affected dorsal root ganglion - a neuromodulatory technique that reduces nerve hypersensitivity without ablation, ideal for disc-related radiculopathy where preserving nerve function is paramount.
- Selective nerve root blocks - diagnostic and therapeutic injections at the specific nerve root level contributing to symptoms, useful when multiple levels are involved.
- Intradiscal RFA (biacuplasty) - for patients where the disc annulus itself is generating pain, this procedure treats the pain-generating disc tissue directly.